
陰莖靜脈滲漏 – 勃起功能障礙的重要原因
以前認為勃起功能障礙的原因大部分是精神性(心理性)因素,後來發現大部分勃起功能障礙的原因是器質性(生理性)因素。器質性因素中,血管性因素、特別是陰莖靜脈血管滲漏因素,扮演最主要的角色。根據統計,陰莖靜脈滲漏的發生比率約佔血管性因素的80%(68-92.5%)。勃起功能障礙其中一個關鍵因素就是陰莖靜脈滲漏。
容易發生陰莖靜脈滲漏的因素包括高血脂、高血壓、糖尿病、海綿體慢性缺氧、陰莖動脈灌流不足、陰莖彎曲、陰莖外傷、佩諾尼氏症、海綿體神經損傷等病因[7,8]。
陰莖靜脈截除手術原理
當開始勃起時,動脈血管擴張、陰莖海綿體內平滑肌放鬆,大量血液經由陰莖動脈灌流進入陰莖海綿體內造成充血膨脹,此時如果陰莖靜脈系統不能完全閉鎖,發生靜脈滲漏,血液將快速流出陰莖海綿體,導致勃起困難、硬度不足或勃起後較快消軟等功能障礙。當然,陰莖靜脈滲漏也有不同程度的差異,勃起硬度就會有所差別,但是目前對於陰莖靜脈滲漏並無程度分級。
陰莖靜脈手術原理即在於截除或綁紮滲漏的陰莖靜脈,阻滯陰莖靜脈血液回流,讓血液不會很快流出陰莖海綿體,使陰莖海綿體內維持充血飽滿狀態,達到足夠從事性行為的勃起硬度。譬如一個茶杯要斟滿水,如果杯底有個破洞,茶杯就不易斟滿;破洞小時,上面多加點水尚可彌補滲漏的部份,維持滿杯的情況(口服藥物即是應用此原理,協助放鬆陰莖動脈及海綿體的平滑肌,增加血液灌流進入陰莖海綿體);然而破洞大時,上面多加水也無濟於事。此時治本之道,就在於手術治療靜脈滲漏。
陰莖靜脈系統
傳統觀念
陰莖靜脈系統在勃起功能中扮演非常重要的角色,但是傳統醫學文獻及解剖教科書對於陰莖靜脈系統解剖構造的解說,只是粗略描述淺背靜脈(superficial dorsal vein)、深背靜脈(deep dorsal vein)、環狀靜脈(circumflex vein)、陰莖腳靜脈及短促的海綿體靜脈(cavernous vein)等的分布情形,實際上並不完整精確(圖1);遺憾的是,當今的解剖或泌尿科學教科書上所描繪的陰莖靜脈系統尚未加以修正。
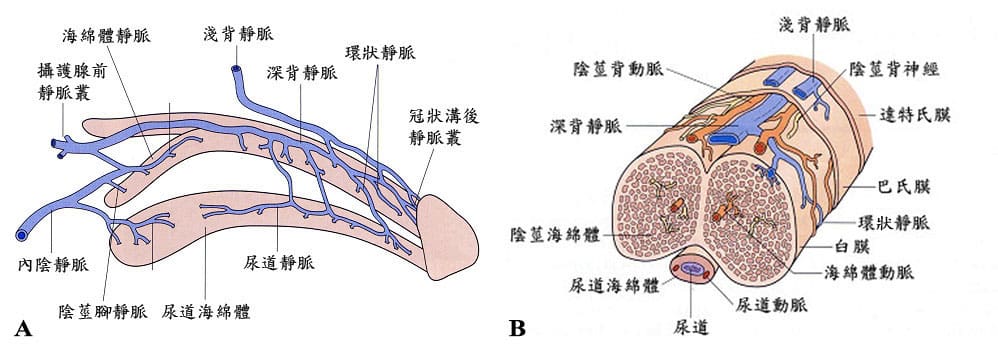
圖1. 傳統醫學文獻及教科書對於陰莖靜脈系統解剖構造的解說並不完整精確,僅是粗略描述淺背靜脈、深背靜脈、環狀靜脈、陰莖腳靜脈(crural vein)及短促的海綿體靜脈。
創新觀念 – 陰莖靜脈系統新發現
1999年國內許教授等發現醫學文獻及解剖教科書上從未曾描述過的靜脈血管,經由反覆的解剖及臨床攝影檢查,掃描式與穿透式電子顯微鏡的輔助,證實陰莖靜脈眾多且複雜,除了以往所描述的深背靜脈(deep dorsal vein)系統、環狀靜脈、陰莖腳靜脈外,還有新發現及命名的海綿體靜脈(cavernosal vein)及動脈旁靜脈(para-arterial vein)兩組系統 。
海綿體靜脈 – 深背靜脈位於陰莖背側正中間;在深背靜脈左右兩側較深處(貼近白膜)各有一條很長的海綿體靜脈,幾乎延伸達到整個陰莖海綿體的長度,並非如傳統醫學文獻及教科書上所描述僅是位於陰莖腳(penile crura)短短的一小段靜脈而已。
動脈旁靜脈 – 在深背靜脈兩側各有一條背動脈,每條背動脈又各被兩條教科書上從未提及的動脈旁靜脈所包夾(一條是內側動脈旁靜脈,另一條是外側動脈旁靜脈) (圖2)。
以上這些靜脈血管匯集來自龜頭、陰莖海綿體的血液後,再流回到體內循環系統。

圖2. 最新發現的詳細陰莖靜脈系統解剖構造圖A.右側視圖,B.橫切面圖。陰莖靜脈系統包括淺背靜脈、深背靜脈位於陰莖背側正中間,在深背靜脈左右兩側較深處各有一條海綿體靜脈,海綿體靜脈很長,幾乎延伸達到整個陰莖海綿體的長度。深背靜脈兩側各有一條背動脈,每條背動脈又各被兩條動脈旁靜脈所包夾。另有環狀靜脈及陰莖腳靜脈。
陰莖靜脈截除手術
傳統的陰莖靜脈截除手術(traditional penile venous surgery)
根據傳統醫學文獻及教科書對於陰莖靜脈系統解剖構造的描述,傳統的陰莖靜脈截除手術主要截除陰莖根部一部分的陰莖深背靜脈,認為如此即可阻滯大部分的陰莖靜脈血液回流,改善勃起功能;然而卻因為未能了解詳盡完整的陰莖靜脈系統分佈,沒有一網打盡其餘勃起相關的靜脈血管,那些未被完全截除或綁紮的殘餘靜脈(residual veins),以前常被誤認為是再生的靜脈(recurrent veins),將慢慢鼓脹成為陰莖靜脈滲漏的來源,逐漸影響患者的勃起功能。
以上情形可以解釋為何盛行於1990年代的陰莖靜脈手術,常因術後追蹤效果不佳而放棄執行此項手術;只有建議手術條件良好(highly selective)的患者才適合接受陰莖靜脈截除手術,包括輕微陰莖靜脈滲漏、無心理性因素或其他器質性因素、服藥效果不佳、只剩下海綿體內藥物注射、真空吸引器或植入人工陰莖治療方式可以選擇的年輕人。因此,詳盡了解陰莖靜脈系統的分佈,據此做為改良式陰莖靜脈截除手術的指引,才能完整處理滲漏的陰莖靜脈。
改良式陰莖靜脈截除手術(refined penile venous stripping surgery)
2005年一項特別針對改良式陰莖靜脈截除手術前後,陰莖海綿體攝影檢查及動態灌流壓力變化的研究報告,研究目的在於排除陰莖勃起受到荷爾蒙、動脈血管、神經、海綿體、藥物和心理等複雜因素造成的交互影響,其結果顯示手術後的海綿體內壓(intracavernous pressure, ICP)升高,較少的血液灌注量即可勃起、縮短達到勃起堅硬所需要的時間。結論為陰莖靜脈系統對於陰莖勃起反應及堅硬程度扮演十分重要的角色。
由於陰莖靜脈系統的觀念更新,進一步發展出改良式陰莖靜脈截除手術。改良式陰莖靜脈截除手術採用局部麻醉方式,更徹底完整綁紮截除深背靜脈、海綿體靜脈、動脈旁靜脈、環狀靜脈、兩側陰莖腳靜脈等陰莖靜脈滲漏相關的靜脈血管,才能達到更好的術後效果。
麻醉方式(Anesthesia)
傳統的陰莖靜脈手術採用半身麻醉或全身麻醉技術,病患術後需住院數日恢復。
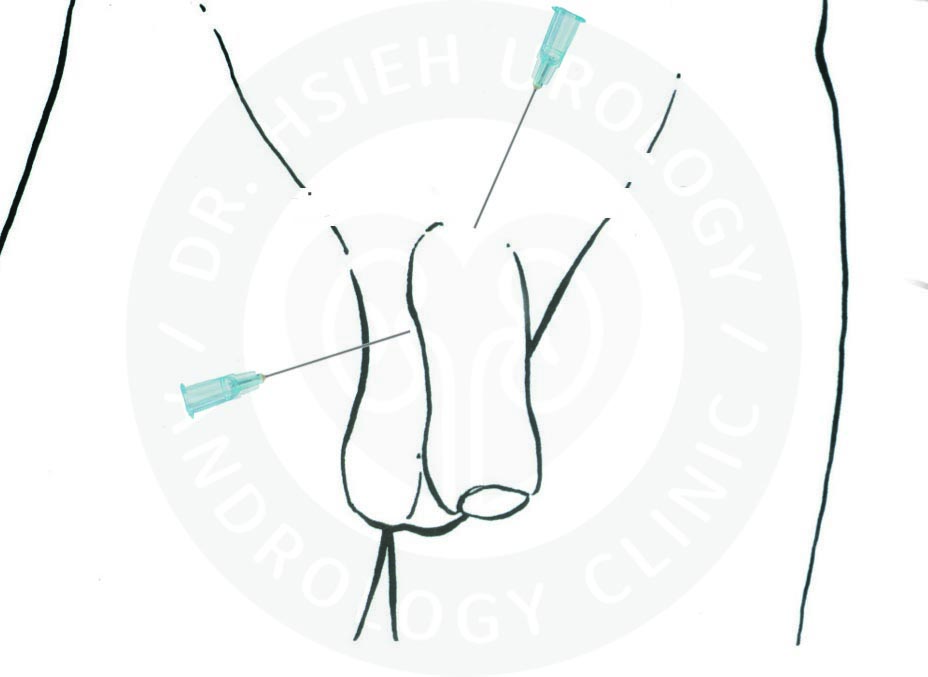
本院執行改良式陰莖靜脈截除手術,採用精準的雙重局部麻醉技術,包括背神經近枝阻斷術(proximal dorsal nerve block)及周陰莖基部組織阻斷(peripenile infiltration),只在陰莖根部注射局部麻醉藥物(圖3),有效麻醉時間約4-6小時,有充足的時間才能完成精細的手術,相對安全又方便,無半身麻醉或全身麻醉的風險。手術過程中清醒不會痛,可滑手機、使用藍芽耳機。手術後不需住院,亦不需要留下觀察,即可自由行走返家休息,甚少影響日常生活及工作。
手術方法(Surgical Technique)
本院以最新了解的陰莖靜脈系統解剖構造,作為執行改良式陰莖靜脈截除手術的指引,完整處理滲漏的陰莖靜脈。患者採平躺姿勢,依照一般手術無菌原則剃除附近毛髮、消毒及鋪上無菌布單。在下恥骨部表皮正中縱切長度約3公分的傷口;如果同時執行包皮環切手術,冠狀溝下將另有一包皮環切傷口。小心游離傷口內面組織(圖4-1),將陰莖本體外翻(圖4-2)。貼近白膜以微細縫線綁紮、完整截除位於陰莖背側正中間的深背靜脈及位於陰莖左右兩側的海綿體靜脈(圖4-3),動脈旁靜脈、環狀靜脈和陰莖腳靜脈等更小的陰莖靜脈血管則以微細縫線綁紮,阻滯陰莖靜脈血液回流。之後將外翻的陰莖本體歸位,以細小縫線縫合傷口完成手術,並立即以紗布纏繞包紮(圖4-4)。 由於此項精細手術須綁紮的靜脈血管部位眾多,甚至高達100餘處,手術時間約需3-6小時。手術過程中需保留陰莖淺背靜脈及球尿道靜脈(bulbourethral vein)以維持陰莖正常的血液循環,因為陰莖淺背靜脈是淺部陰莖組織所需血液回流的管道,而球尿道靜脈負責深部組織的循環。

精細的改良式陰莖靜脈截除手術出血極微量,不需使用電燒止血,組織破壞最少。由於陰莖的體積不大,血管與神經系統相當接近,手術中如果使用電燒止血,可能熱傷害到緊鄰的陰莖背動脈、背神經叢或周圍組織,造成神經感覺異常、麻木感或慢性疼痛、局部組織缺血壞死或勃起功能障礙(陽痿)。許多醫學文獻報告指出,使用電燒止血時,局部組織遭到破壞,止血燒焦的地方無血液循環,對細菌的抵抗力下降,將增加傷口感染發炎的機率;即使沒有發炎感染,也易影響傷口較難癒合。改良式陰莖靜脈截除手術過程中如偶遇小出血點,不使用電燒止血,而採用微細縫線綁紮止血,以避免造成鄰近組織、動脈血管及神經的熱傷害,減少可能的併發症。
手術結果
執行傳統陰莖靜脈手術,有文獻報告術後三個月內,93.3%患者有良好的勃起反應,追蹤兩年40%患者仍有自發性勃起。Wespes等人報告50%謹慎選擇的病人在切除深背靜脈後恢復勃起功能。Cayan報告26位病人因陰莖靜脈切除手術而獲益,術後追蹤12個月以上,國際勃起功能指標在生物統計學上有顯著改善。Flores等人直接綁紮相關的陰莖靜脈,治療先天性或外傷後病變引起的單獨靜脈滲漏效果良好。
傳統陰莖靜脈手術早期報告短期結果令人鼓舞,短期追蹤改善的比率約50-80%;然而,長期追蹤改善的比率約31-64%。追蹤改善比率隨著長期追蹤而降低,可能的原因包括陰莖靜脈截除綁紮不完整、海綿體間血液滲漏、海綿體平滑肌功能障礙、不明血管病變、選擇的患者手術條件不佳、有潛在疾病或年齡逐漸老化等因素。
先前曾接受傳統的靜脈手術,但是勃起功能仍然不佳的患者,如採用改良式陰莖靜脈截除手術進行挽救,也有不錯的改善效果,推論即因接受傳統的陰莖靜脈手術的患者,尚有許多未被完全綁紮截除的殘餘靜脈,慢慢鼓脹成為陰莖靜脈滲漏的來源,而非靜脈再生的結果,以至於逐漸影響勃起功能,術後改善程度有限,長期追蹤效果不佳。
如果謹慎選擇手術條件良好患者,採用改良式陰莖靜脈截除手術,長期追蹤結果90.4%報告有進步,國際勃起功能指標在生物統計學上有顯著改善,另一研究報告滿意度可達87.9%。傳統的陰莖靜脈截除手術,文獻報告可能發生的併發症包括血腫、感染、麻木感、包皮局部缺血壞死等,但是只要熟練精細手術技巧,發生機率極低。採用改良式陰莖靜脈截除手術,僅有輕微併發症,包括可能的暫時性淋巴水腫、皮下瘀青、局部麻醉引起短暫性心悸等;長期追蹤報告,則無發生相關的重大併發症。
評論
勃起功能障礙有許多不同的原因,常是複合性因素所造成,患者可能同時存在許多其他疾病及病因,陰莖靜脈滲漏是其中一個重要的關鍵因素,但是目前醫學上沒有任何單一療法可以完全治癒所有的勃起功能障礙。許多專家學者質疑陰莖靜脈手術不能解決潛在的諸多病因,因而放棄此項手術作為勃起功能障礙的治療選擇;美國泌尿科醫學會(AUA)及歐洲泌尿科醫學會(EUA)關於勃起功能障礙的治療指南,亦不建議執行陰莖靜脈手術。令人困惑的是,同樣的擔憂質疑應該同樣適用於各醫學會治療指南中的各項治療選擇,因為當前所推薦的其他治療選項,同樣無任何一個選項能夠完全解決勃起功能障礙潛在的諸多病因。
陰莖靜脈滲漏是勃起功能障礙的一項重要關鍵因素,在更深入了解陰莖靜脈解剖結構的情況下,改良式陰莖靜脈截除手術的術後勃起功能,其改善程度優於傳統的陰莖靜脈手術,這在臨床經驗上已獲得印證,近期文獻報告的追蹤結果亦顯示此一趨勢,對於謹慎選擇的陰莖靜脈滲漏患者有極佳助益。將陰莖靜脈手術整合到目標導向的治療選項中,包括心理諮詢、藥物(例如磷酸二酯酶抑製劑和陰莖海綿體注射)、非手術方式(例如低能量體外震波)和替代手術(例如人工陰莖植入手術),才能讓目標導向的治療策略最佳化。
結語
雙重局部麻醉下執行改良式陰莖靜脈手術,仍然是治療勃起功能障礙可行且重要的治療選擇,提供改善勃起功能的機會;對於謹慎選擇手術條件良好的靜脈血管滲漏患者仍有助益,可能獲得自發性、不需其他方法協助且自然的勃起,具有安全、有效、可靠、方便等特點。精細熟練的手術技巧則能避免可能發生的併發症。手術後不需留下觀察,即可自由行走返家休息,患者隱私更有保障,更早恢復日常生活及工作,是最自然的治療方法之一!
每位患者體質及手術條件不一,即使術後效果因人而異,勃起功能大多會有不同程度的改善。即使術後勃起功能尚有不足,仍可搭配併用其它治療方法,例如口服藥物,加強輔助改善勃起功能。最後,如果所有的其他治療方法都失效,患者仍有機會選擇人工陰莖植入手術。
期刊論文
- Hsu GL(許耕榕), Hsieh CH(謝政興), Chen HS, Ling PY, Wen HS, Liu LJ, Chen CW, Chua C. The advancement of pure local anesthesia for penile surgeries: can an outpatient basis be sustainable (純粹局部麻醉施行陰莖手術的新進展). Journal of Andrology. 28(1):200-205, 2007.
- Hsu GL, Zaid UX, Hsieh CH (謝政興), Huang SJ. Acupuncture assisted local anesthesia for penile surgeries (針灸輔助局部麻醉下施行陰莖手術). Translational Andrology and Urology. 2(4):291-300, 2013.
- Hsu GL(許耕榕), Hsieh CH(謝政興), Wen HS, Hsu WL, Chen YC, Chen RM, Chen SC, Hsieh JT. The effect of electrocoagulation on the sinusoids in the human penis (電燒止血對於人類陰莖海綿體的影響). Journal of Andrology. 25(6):954-959, 2004.
- Hsu GL(許耕榕), Hsieh CH(謝政興), Wen HS, Chiang HS. Penile venous anatomy: application to surgery for erectile disturbance (陰莖靜脈解剖構造:在勃起功能障礙手術中的應用). Asian Journal of Andrology. 4(1):61-66, 2002.
- Hsu GL(許耕榕), Hsieh CH(謝政興), Wen HS, Chen YC, Chen SC, Mok MS. Penile venous anatomy: an additional description and its clinical implication (陰莖靜脈解剖構造:附加描述及其臨床意涵). J Androl. 2003; 24: 921-927.
- Hsu GL(許耕榕), Hsieh CH(謝政興), Wen HS, Hsu WL, Wu CH, Fong TH, Chen SC, Tseng GF. Anatomy of the human penis: the relationship of the architecture between skeletal and smooth muscles (人類陰莖解剖構造:骨骼肌和平滑肌之間的結構關係). Journal of Andrology. 25:426-431, 2004.
- Hsieh CH(謝政興), Wang CJ, Hsu GL(許耕榕), Chen SC, Ling PY, Wang T, Fong TH, Tseng GF. Penile veins play a pivotal role in erection: the hemodynamic evidence (陰莖靜脈在勃起中扮演關鍵角色:血液動力學上的證據). International Journal of Andrology. 28(2):88-92, 2005.
- Chen SC, Hsieh CH(謝政興), Hsu GL(許耕榕), Wang CJ, Wen HS, Ling PY, Huang HM, Tseng GF. The progression of the penile vein: could it be recurrent (陰莖靜脈的進展:陰莖靜脈手術後是否會復發)? Journal of Andrology. 26(1):53-60, 2005.
- Wen HS, Hsieh CH(謝政興), Hsu GL(許耕榕), Kao YC, Ling PY, Huang HM, Wang CJ, Einhorn EF. The synergism of penile venous surgery and oral sildenafil in treating patients with erectile dysfunction (陰莖靜脈截除手術與口服威而剛治療勃起功能障礙的協同作用). International Journal of Andrology. 28(5):297-303, 2005.
- Hsu GL(許耕榕), Chen HS, Hsieh CH(謝政興), Lin PL, Wen HS, Liu LJ, Chen CW, Liu MW. Insufficient response to venous stripping surgery: is the penile vein recurrent or residual (陰莖靜脈截除手術後反應不佳:陰莖靜脈復發或殘留?). Journal of Andrology. 27(5):700-706, 2006.
- Hsu GL(許耕榕), Chen HS, Hsieh CH(謝政興), Lee WY, Chen KL and Chang CH. Salvaging penile venous stripping surgery (陰莖靜脈截除挽救手術). Journal of Andrology. 31(3):250-260, 2010.
- Hsu GL(許耕榕), Chen HS, Hsieh CH(謝政興), Lee WY, Chen KL and Chang CH. Clinical experience of a refined penile venous stripping surgery procedure for patients with erectile dysfunction: is it a viable option (精煉的改良式陰莖靜脈截除手術治療勃起功能障礙的臨床經驗:手術是可行的選擇?). Journal of Andrology. 31(3):271-280, 2010.
- Hsu GL(許耕榕), Hung YP, Tsai MH, Hsieh CH(謝政興), Chen HS, Molodysky E, Huynh CC, Yu HJ. Penile veins are the principal component in erectile rigidity: a study of penile venous stripping on defrosted human cadaver (陰莖靜脈是達成勃起硬度的主要因素:在解凍的人類屍體上進行陰莖靜脈截除手術的研究). Journal of Andrology. 33:1176-1185, 2012.
- Hsieh CH(謝政興), Hsieh JT, Chang SJ, Chiang IN, Yang SSD. Penile venous surgery for treating erectile dysfunction: past, present, and future perspectives with regard to new insights in venous anatomy (陰莖靜脈手術治療勃起功能障礙的過去、現在與未來:陰莖靜脈解剖學的新見解). Urological Science. 27(2):60-65, 2016.
- Hsieh CH(謝政興), Hsu GL(許耕榕), Chang SJ, Yang SSD, Liu SP, Hsieh JT. Surgical niche for the treatment of erectile dysfunction (手術治療勃起功能障礙的利基). International Journal of Urology. 2020; 27: 117-133.
書籍著作
- Cheng-Hsing Hsieh (謝政興), Geng-Long Hsu. Current role of vascular surgery (arterial and venous) in erectile dysfunction (當前動脈及靜脈血管手術在勃起功能障礙中的角色), in INTERNATIONAL BOOK OF ERECTILE DYSFUNCTION, M.L. Djordjevic and F.E. Martins, Editors. 2016, Nova Science Publishers, Inc.: New York. chap. 9, pp. 129-157. ISBN: 978-1-63485-289-0
- Geng-Long Hsu, Cheng-Hsing Hsieh (謝政興), Eric Allaire. Vascular (Arterial and Venous) Surgery for Erectile Dysfunction (血管(動脈與靜脈)手術治療勃起功能障礙), in Textbook of Male Genitourethral Reconstruction, Francisco E. Martins, Sanjay B. Kulkarni and Tobias S. Köhler, Editors. 2020, Springer Nature: Switzerland AG. chap. 50, pp. 663-678. ISBN: 978-3030214463
- Cheng-Hsing Hsieh (謝政興)、Geng-Long Hsu (許耕榕). 治療勃起功能障礙 – 手術治療(Erectile Dysfunction – Surgical Management).書名:男性性功能障礙 – 臨床診治全攻略 (Male Sexual Dysfunction – A Complete Guide to Diagnosis and Treatment), 陳煜、簡邦平、蔡維恭、陳卷書編輯. 合記圖書出版社, 2023. 第三篇,第17章,頁245-262.
- Cheng-Hsing Hsieh (謝政興)、Geng-Long Hsu (許耕榕). 勃起功能障礙 – 手術治療 (Erectile Dysfunction – Surgical Treatment). 書名:臨床泌尿學 (CLINICAL UROLOGY).郭漢崇、賴明坤、楊啟瑞、黃一勝、余燦榮、陳進典、崔克宏,編輯. 台灣泌尿科醫學會, 2012.第八篇,第54章,頁1037-1049.
- Geng-Long Hsu (許耕榕)、Cheng-Hsing Hsieh (謝政興). 書名:A LABORATORY MANUAL FOR POTENCY MICROSURGERY (性功能顯微手術實驗訓練手冊). 許耕榕、謝政興,編輯.
參考文獻
- Das S. Early history of venogenic impotence. Int J Impot Res. 1994; 6: 183–189.
- Wespes E, Schulman CC. Venous leakage: surgical treatment of a curable cause of impotence. J Urol. 1985; 133: 796-798.
- Lue TF. Penile venous surgery. Urol Clin North Am. 1989; 16: 607-611.
- Lue TF. Surgery for crural venous leakage. Urology. 1999; 54: 739-741.
- Bennett AH, Rivard DJ, Blanc RP, Moran M. Reconstructive surgery for vasculogenic impotence. J Urol. 1986; 136: 599-601.
- Berardinucci D, Morales A, Heaton JP, Bloom S. Surgical treatment of penile veno-occlusive dysfunction: is it justified? Urology. 1996; 47: 88-92.
- Montague DK, Barada JH, Belker AM, et al. Clinical guidelines panel on erectile dysfunction: summary report on the treatment of organic erectile dysfunction. The American Urological Association. J Urol. 1996; 156: 2007-2011.
- Hsu GL, Hsieh CH, Wen HS, Chen YC, Chen SC, Mok MS. Penile venous anatomy: an additional description and its clinical implication. J Androl. 2003; 24: 921–927.
- Hsu GL, Hung YP, Tsai MH, et al. Penile veins are the principal component in erectile rigidity: a study of penile venous stripping on defrosted human cadavers. J Androl. 2012; 33: 1176-1185.
- Hsu GL, Chen HS, Hsieh CH, Lee WY, Chen KL, Chang CH. Clinical experience of a refined penile venous stripping surgery procedure for patients with erectile dysfunction: is it a viable option? J Androl. 2010; 31: 271-280.
- Hsieh CH, Hsu GL, Chang SJ, Yang SSD, Liu SP, Hsieh JT. Surgical niche for the treatment of erectile dysfunction. Int J Urol. 2020; 27: 117-133.
- Hwang TI, Yang CR. Penile vein ligation for venogenic impotence. Eur Urol. 1994; 26: 46.
- Hsu GL, Chen HS, Hsieh CH, et al. Insufficient response to venous stripping surgery: is the penile vein recurrent or residual? J Androl. 2006; 27: 700-706.