
Inguinal hernia, also known as groin hernia, is a common urological disease. The inguinal canal is a sloping channel located near the junction of the abdomen and thigh, through which the spermatic cord passes in males and the round ligament of the uterus passes in females. Inguinal hernia is characterized by an abnormal bulge in the inguinal region on either side (see Figure 1).
Inguinal hernia and classification:
There are several classification systems for inguinal hernia, but the Nyhus classification system is the most commonly referenced. It includes the following types:
Type I: Indirect inguinal hernia. The internal ring of the inguinal canal is normal (as in pediatric hernias).
Type II: Indirect inguinal hernia. The internal ring of the inguinal canal is enlarged, but the posterior wall of the inguinal canal is intact.
Type III: Weakness of the posterior wall of the inguinal canal, including the following subtypes:
- Type III A: Direct inguinal hernia with a defect in the posterior wall of the inguinal canal.
- Type III B: Indirect inguinal hernia with an enlarged internal ring (such as a large scrotal hernia or sliding hernia) and weakness in the posterior wall of the inguinal canal.
- Type III C: Femoral hernia.
Type IV: Recurrent hernia, including the following subtypes:
- Type IV A: Direct inguinal hernia.
- Type IV B: Indirect inguinal hernia.
- Type IV C: Femoral hernia.
- Type IV D: All three types of hernias (direct, indirect, and femoral) are present.
If we disregard the complex classification system, inguinal hernias can be simply divided into indirect and direct hernias based on their underlying causes.
Indirect inguinal hernias (congenital hernias) (see Figure 1)
Can occur at any age (from newborns to the elderly), but are particularly common in infants. In full-term infants, the incidence is about 1-5%, while in premature infants it is higher (9-11%). The incidence in males is 3:1 to 10:1 higher than that in females, and about 60% occur on the right side, 30% on the left, and 10% on both sides. Many patients have a family history of hernia, but there is no specific inheritance pattern.
During embryonic development, children have a tubular protrusion of the peritoneum called the processus vaginalis, which extends from the abdominal cavity to the abdominal wall and runs alongside the spermatic cord (in males) or round ligament of the uterus (in females). Shortly after birth, this channel should naturally close; however, if it remains open, it will result in a connected hernia sac between the abdominal cavity and abdominal wall, and even into the scrotum, causing a hernia. Organs such as the intestines, ovaries, or omentum in the abdominal cavity may enter the hernia sac and pass through the inguinal canal into the abdominal wall, causing it to bulge, or even into the scrotum, causing scrotal swelling (although this rarely extends to the labia in females). Hydrocele is also caused by the incomplete closure of the processus vaginalis, but the sac usually contains fluid rather than organs from the abdominal cavity.
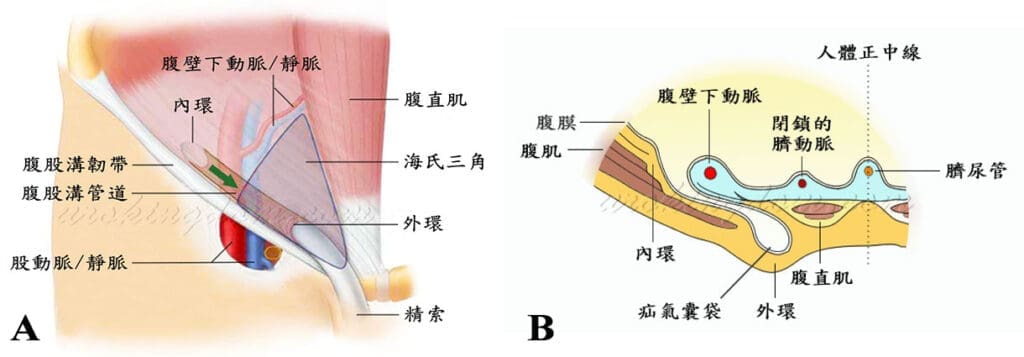
Figure 2: Illustration of direct inguinal hernia (acquired hernia).
The inguinal triangle of Hesselbach, which is formed by the lateral border of the rectus abdominis muscle, the inguinal ligament, and the inferior epigastric vessels, is the weakest area of the anterior abdominal wall and can be further weakened by aging. Increased abdominal pressure caused by conditions or diseases such as intra-abdominal tumors, heart failure, chronic cough due to COPD, enlarged prostate requiring straining during urination, constipation, or heavy lifting can lead to the gradual protrusion of weakened abdominal wall tissue and the formation of an abnormal bulge in the inguinal canal, resulting in a direct inguinal hernia.
